
BPD and Opioid Use Disorder (OUD)
Estimates suggest as many as one in every 10 people with BPD dies by suicide (Temes et al., 2019; Girardi et al., 2022).
Individuals with OUD are 14 times more likely to die by suicide relative to the general population, and opioids are found in 20% people who dies by suicide in the US. Alarmingly, risk is even higher when people with BPD use opioids (Arregui et al., 1992; Temes et al., 2019). BPD is associated with a greater quantity and frequency of opioid use, increased risk for analgesic misuse, and markedly elevated rates of comorbid OUD (Tragesser et al., 2010). Moreover, a comorbid BPD diagnosis (observed in 19-44% of individuals with OUD) (Trull et al., 2010; Darke et al., 2004; Darke et al., 2005; Darke et al., 2007; Trull et al., 2007) is associated with more severe and persistent symptom presentation in both disorders, and a significantly higher likelihood of adverse consequences (Hasin et al., 2011; Campbell et al., 2015) (including death by overdose and suicide) (Maloney et al., 2009).
Despite the complexity and seriousness of these highly comorbid disorders, available agents largely fall short of affecting overall symptom severity BPD-OUD (Ripoll, 2013, Lieb et al., 2010, & Hancock-Johnson et al., 2017) and no available treatments reliably reduce suicide risk in this population.
Therefore, understanding the pathophysiology of BPD-OUD is crucial to the development of potentially life-saving interventions tailored to this high-risk population.
Recent evidence supports a role for the kappa opioid system (KOR) in the pathophysiology and maintenance of BPD, OUD, and their comorbid presentation. The opioid system is instrumental in the regulation of core features of BPD-OUD, including impulsivity (New et al., 2010), social functioning (Kennedy et al., 2006), and the experience of pain (Agren et al., 1991). Evidence from both human (Pietrzak et al., 2014) and preclinical (Knoll et al., 2010, Chartoff et al., 2012, Peters et al., 2011) studies suggests KOR signaling mediates the effect of stress on the development of psychiatric symptoms (Knoll et al., 2010; Anderson et al., 2019) including addiction (Metcalf & Coop, 2008). Elevated dynorphin (a KOR-associated opioid peptide), which can result from chronic stress (Esterlis et al., 2017), and agonism of KOR are both associated with symptoms of BPD-OUD (e.g., dissociation (Walsh et al., 2001) or cognitive dysfunction (Bruchas et al., 2010)). Similarly, preclinical studies show KOR involvement in impulsive behavior and social dysfunction (Knoll et al., 2010 & Bruchas et al., 2011). Further, postmortem work has linked KOR expression (Hurd et al., 1997 & Lutz et al., 2018) including lower KOR availability in the amygdala (Hurd, 2002) and anterior cingulate (ACC) (Lutz et al., 2018) specifically to suicide mortality.
Clinical trials of KOR antagonists are underway in BPD and ongoing in OUD; unfortunately, those with BPD-OUD remain understudied and are frequently excluded from clinical trials due to risk and clinical complexity.
Thus, there is strong support for KOR as a potential target in BPD-OUD. However, the role and clinical relevance of KOR in BPD-OUD is not yet well understood.
Our goals for this study include:
Determining whether comorbid presentation of BPD-OUD is associated with lower KOR availability.
Determining whether history of suicide behavior is associated with lower KOR availability in BPD-OUD.
Examining the association between KOR availability and other endophenotypic correlates of suicide risk in BPD-OUD: impulsivity, and pain sensitivity.
Suggested reading:
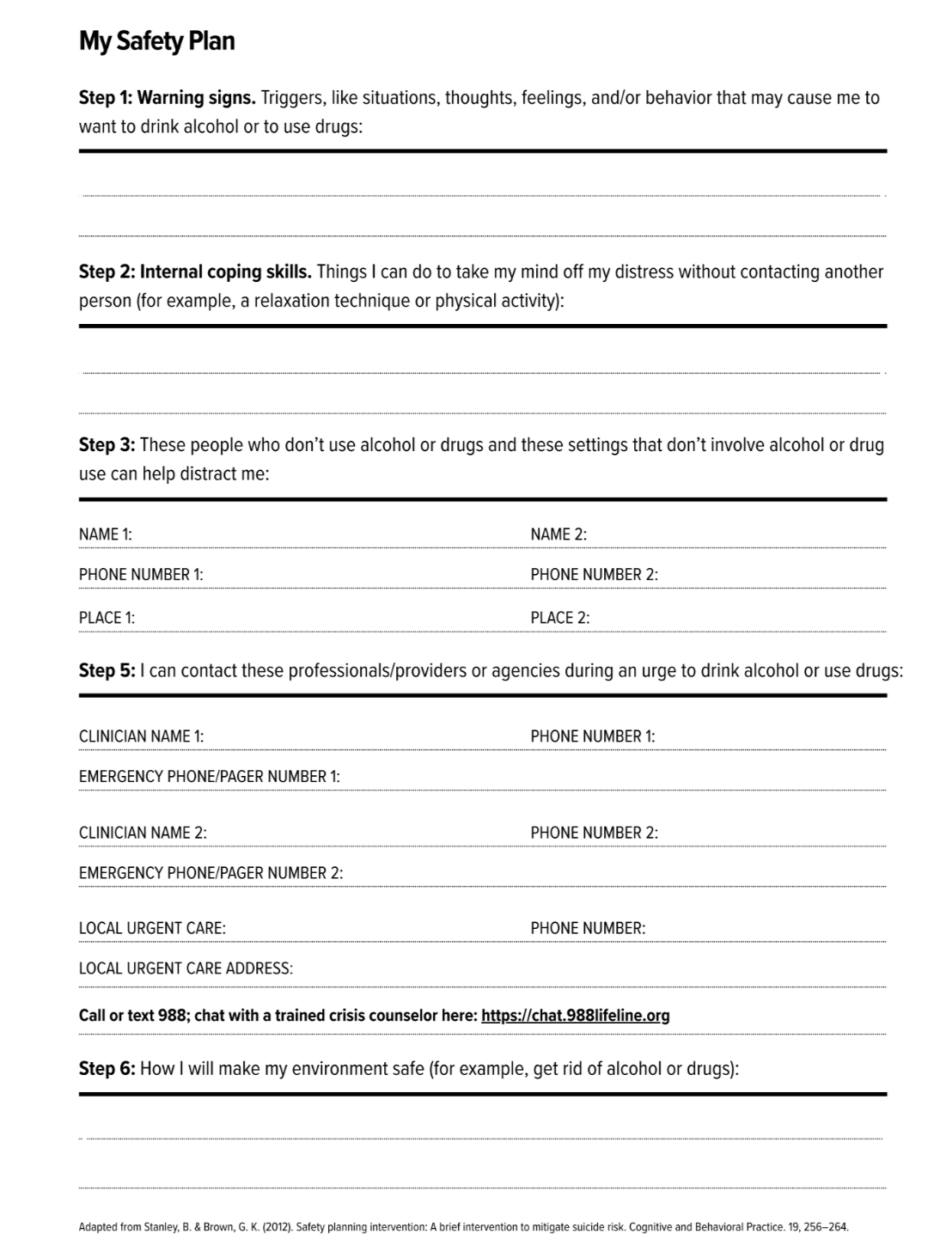
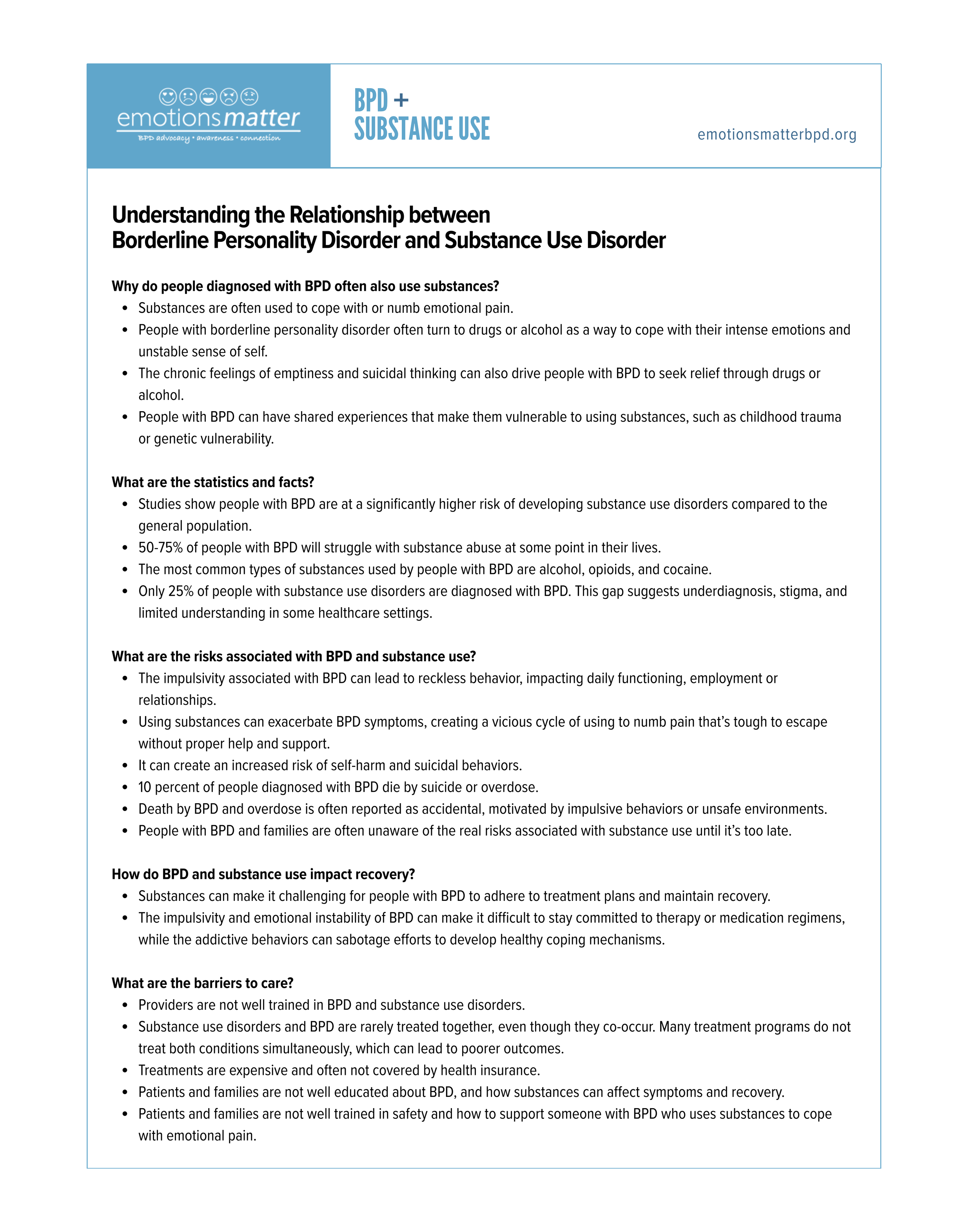
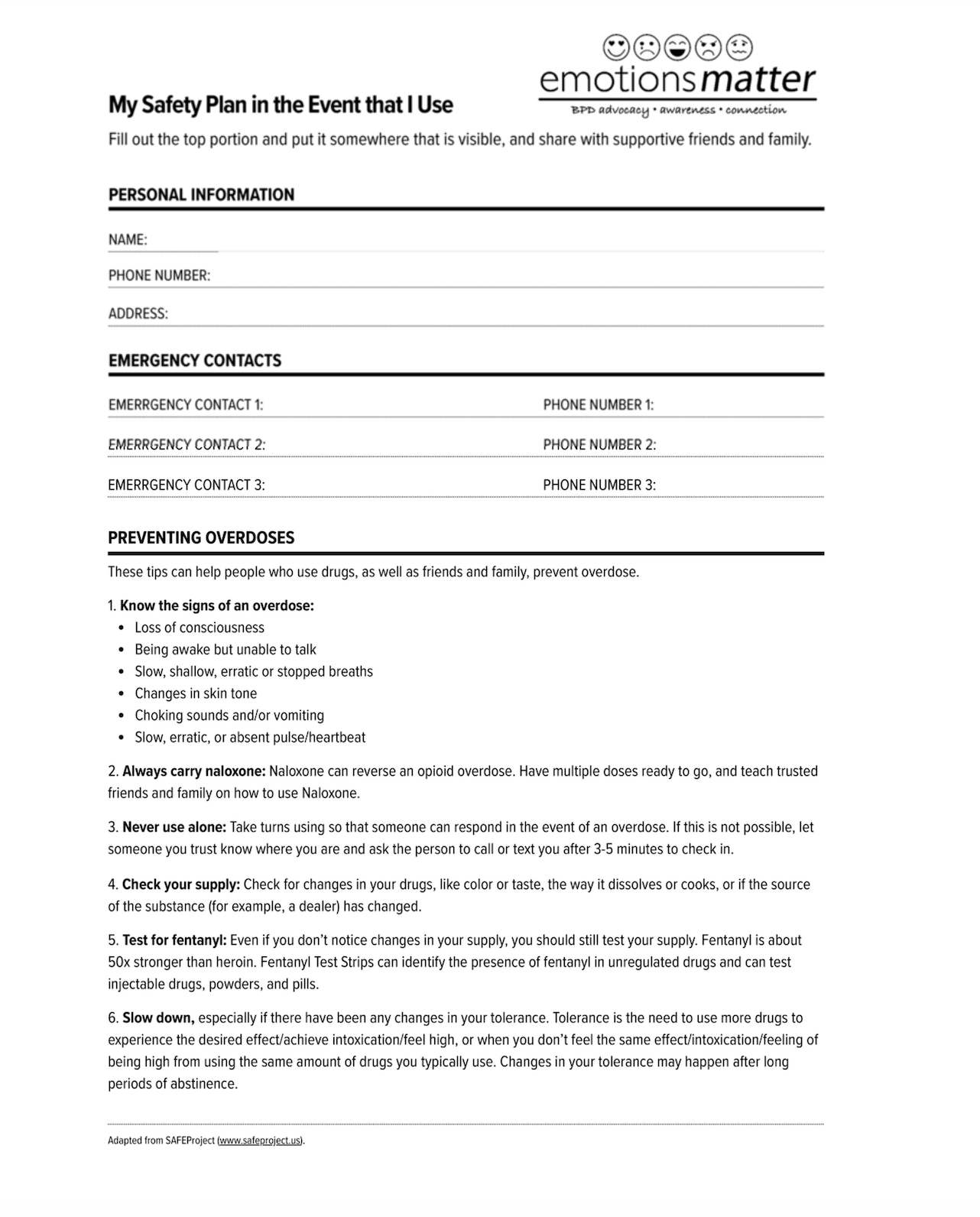
Resources

Citations
Temes CM, Frankenburg FR, Fitzmaurice GM, Zanarini MC. Deaths by suicide and other causes among patients with borderline personality disorder and personality-disordered comparison subjects over 24 years of prospective follow-up. The Journal of clinical psychiatry. 2019;80(1):0-0.
Girardi P, Boldrini T, Braggion M, Schievano E, Amaddeo F, Fedeli U. Suicide mortality among psychiatric patients in Northeast Italy: a 10-year cohort study. Epidemiology and psychiatric sciences. 2022;31.
Trull TJ, Jahng S, Tomko RL, Wood PK, Sher KJ. Revised NESARC personality disorder diagnoses: gender, prevalence, and comorbidity with substance dependence disorders. Journal of personality disorders. 2010;24(4):412-426.
Darke S, Ross J, Williamson A, Mills KL, Havard A, Teesson M. Borderline personality disorder and persistently elevated levels of risk in 36-month outcomes for the treatment of heroin dependence. Addiction. 2007;102(7):1140-1146.
Darke S, Ross J, Williamson A, Teesson M. The impact of borderline personality disorder on 12-month outcomes for the treatment of heroin dependence. Addiction. 2005;100(8):1121-1130.
Darke S, Williamson A, Ross J, Teesson M, Lynskey M. Borderline personality disorder, antisocial personality disorder and risk-taking among heroin users: findings from the Australian Treatment Outcome Study (ATOS). Drug and Alcohol Dependence. 2004;74(1):77-83.
Trull TJ, Sher KJ, Minks-Brown C, Durbin J, Burr R. Borderline personality disorder and substance use disorders: A review and integration. Clinical psychology review. 2000;20(2):235-253.
Hasin D, Fenton MC, Skodol A, Krueger R, Keyes K, Geier T, Greenstein E, Blanco C, Grant B. Personality disorders and the 3-year course of alcohol, drug, and nicotine use disorders. Archives of general psychiatry. 2011;68(11):1158-1167.
Campbell G, Bruno R, Darke S, Degenhardt L. Associations of borderline personality with pain, problems with medications and suicidality in a community sample of chronic non-cancer pain patients prescribed opioids for pain. General hospital psychiatry. 2015;37(5):434-440.
Maloney E, Degenhardt L, Darke S, Nelson EC. Impulsivity and borderline personality as risk factors for suicide attempts among opioid-dependent individuals. Psychiatry research. 2009;169(1):16-21.
Knoll AT, Carlezon Jr WA. Dynorphin, stress, and depression. Brain research. 2010;1314:56-73.
Anderson G. Pathoetiology and pathophysiology of borderline personality: Role of prenatal factors, gut microbiome, mu-and kappa-opioid receptors in amygdala-PFC interactions. Progress in Neuro-Psychopharmacology and Biological Psychiatry. 2019:109782.
Metcalf MD, Coop A. Kappa opioid antagonists: past successes and future prospects. Drug Addiction: Springer; 2008:395-431.
Arregui ME, Davis CJ, Yucel O, Nagan RF. Laparoscopic mesh repair of inguinal hernia using a preperitoneal approach: a preliminary report. Surg Laparosc Endosc. 1992;2(1):53-58.
Tragesser SL, Bruns D, Disorbio JM. Borderline personality disorder features and pain: the mediating role of negative affect in a pain patient sample. The Clinical Journal of Pain. 2010;26(4):348-353.
Ripoll LH. Psychopharmacologic treatment of borderline personality disorder. Dialogues in clinical neuroscience. 2013;15(2):213.
Lieb K, Völlm B, Rücker G, Timmer A, Stoffers JM. Pharmacotherapy for borderline personality disorder: Cochrane systematic review of randomised trials. The British Journal of Psychiatry. 2010;196(1):4-12.
Hancock-Johnson E, Griffiths C, Picchioni M. A Focused Systematic Review of Pharmacological Treatment for Borderline Personality Disorder. CNS drugs. 2017;5(31):345-356.
New AS, Stanley B. An opioid deficit in borderline personality disorder: self-cutting, substance abuse, and social dysfunction: Am Psychiatric Assoc; 2010.
Kennedy SE, Koeppe RA, Young EA, Zubieta J-K. Dysregulation of endogenous opioid emotion regulation circuitry in major depression in women. Archives of general psychiatry. 2006;63(11):1199-
Agren H, Reibring L, Hartvig P, Tedroff J, Bjurling P, Hörnfeldt K, Andersson Y, Lundqvist H, Lângström B. Low brain uptake of L-[11C] 5-hydroxytryptophan in major depression: a positron emission tomography study on patients and healthy volunteers. Acta Psychiatrica Scandinavica. 1991;83(6):449-455.
Pietrzak RH, Naganawa M, Huang Y, Corsi-Travali S, Zheng M-Q, Stein MB, Henry S, Lim K, Ropchan J, Lin S-f. Association of in vivo κ-opioid receptor availability and the transdiagnostic dimensional expression of trauma-related psychopathology. JAMA psychiatry. 2014;71(11):1262-1270.
Chartoff E, Sawyer A, Rachlin A, Potter D, Pliakas A, Carlezon WA. Blockade of kappa opioid receptors attenuates the development of depressive-like behaviors induced by cocaine withdrawal in rats. Neuropharmacology. 2012;62(1):167-176.
Peters MF, Zacco A, Gordon J, Maciag CM, Litwin LC, Thompson C, Schroeder P, Sygowski LA, Piser TM, Brugel TA. Identification of short-acting κ-opioid receptor antagonists with anxiolytic-like activity. European journal of pharmacology. 2011;661(1-3):27-34.
Esterlis I, DellaGioia N, Pietrzak R, Matuskey D, Nabulsi N, Abdallah C, Yang J, Pittenger C, Sanacora G, Krystal J. Ketamine-induced reduction in mGluR5 availability is associated with an antidepressant response: an [11C] ABP688 and PET imaging study in depression. Molecular Psychiatry. 2017.
Walsh SL, Strain EC, Abreu ME, Bigelow GE. Enadoline, a selective kappa opioid agonist: comparison with butorphanol and hydromorphone in humans. Psychopharmacology. 2001;157(2):151-162.
Bruchas M, Land B, Chavkin C. The dynorphin/kappa opioid system as a modulator of stress-induced and pro-addictive behaviors. Brain research. 2010;1314:44-55.
Bruchas MR, Schindler AG, Shankar H, Messinger DI, Miyatake M, Land BB, Lemos JC, Hagan CE, Neumaier JF, Quintana A. Selective p38α MAPK deletion in serotonergic neurons produces stress resilience in models of depression and addiction. Neuron. 2011;71(3):498-511.
Hurd Y, Herman M, Hyde T, Bigelow L, Weinberger D, Kleinman J. Prodynorphin mRNA expression is increased in the patch vs matrix compartment of the caudate nucleus in suicide subjects. Molecular psychiatry. 1997;2(6):495.
Lutz PE, Courtet P, Calati R. The opioid system and the social brain: implications for depression and suicide. Journal of neuroscience research. 2018.
Hurd Y. Subjects with major depression or bipolar disorder show reduction of prodynorphin mRNA expression in discrete nuclei of the amygdaloid complex. Molecular psychiatry. 2002;7(1):75.
Lutz PE, Gross JA, Dhir SK, Maussion G, Yang J, Bramoulle A, Meaney MJ, Turecki G. Epigenetic regulation of the kappa opioid receptor by child abuse. Biological psychiatry. 2018;84(10):751-761.
This study is possible thanks to support from the Yale Biomedical Imaging Institute.
